Kiran (name changed), my brother's former classmate, used to stand at our door as a schoolgirl, calling out his name and asking to borrow his notebook so she could finish her homework. When they changed schools, we gradually lost touch.
Last year, however, she returned carrying a bag filled with blood reports and CT scans. The familiar smile I remembered from childhood had been replaced by fear and quiet vulnerability.
Her mother had recently been diagnosed with advanced-stage gallbladder cancer, an aggressive malignancy that disproportionately affects North India and is sometimes referred to as the "Indian disease." In our neighbourhood, she was affectionately known as Lambi Bhabi, remembered for her radiant smile, her love for Pahadi songs, and her presence at local gatherings.
The diagnosis came as a shock. By the time the cancer was detected, it had already reached an advanced stage and was further complicated by severe jaundice.
Kiran came seeking guidance because my family had walked a similar path. Nine years earlier, my own mother had been diagnosed with the same cancer, received treatment in Delhi, and survived against the odds.
Despite being part of the healthcare workforce herself, Kiran found the journey overwhelming. She travelled across states and hospitals, navigating a maze of consultations before her mother could finally begin treatment.

But Lambi Bhabi was not as fortunate as my mother. She eventually passed away after an exhausting battle, not only with the disease but also with a healthcare system that failed to diagnose it early or provide timely and comprehensive care.
Sadly, her story is not an isolated tragedy. Almost every visit to my hometown now brings news of another cancer diagnosis or another life lost to the disease. Families speak of late-stage detection, long journeys for treatment, financial hardship, and the absence of adequate cancer care closer to home. Survival stories remain rare.
These experiences raise an uncomfortable question: Is Uttarakhand prepared to deal with the growing burden of cancer?
India, the world's third-largest economy, is witnessing a rapid rise in non-communicable diseases, with cancer emerging as one of the country's most serious public health challenges. Nearly 1.9 to 2 million new cancer cases are reported annually, making India one of the largest contributors to the global cancer burden.
While the Union government has launched several initiatives to address this crisis, cancer patterns vary significantly across regions because of differences in lifestyle, environment, and genetic factors. These variations require state-specific responses rather than a one-size-fits-all approach.
As a resident of Uttarakhand, I wanted to understand how prepared the state is to confront this growing challenge. Over the last six to seven months, I filed multiple applications under the Right to Information (RTI) Act, examined available reports, and met officials in the State Health Department while pursuing my appeals.
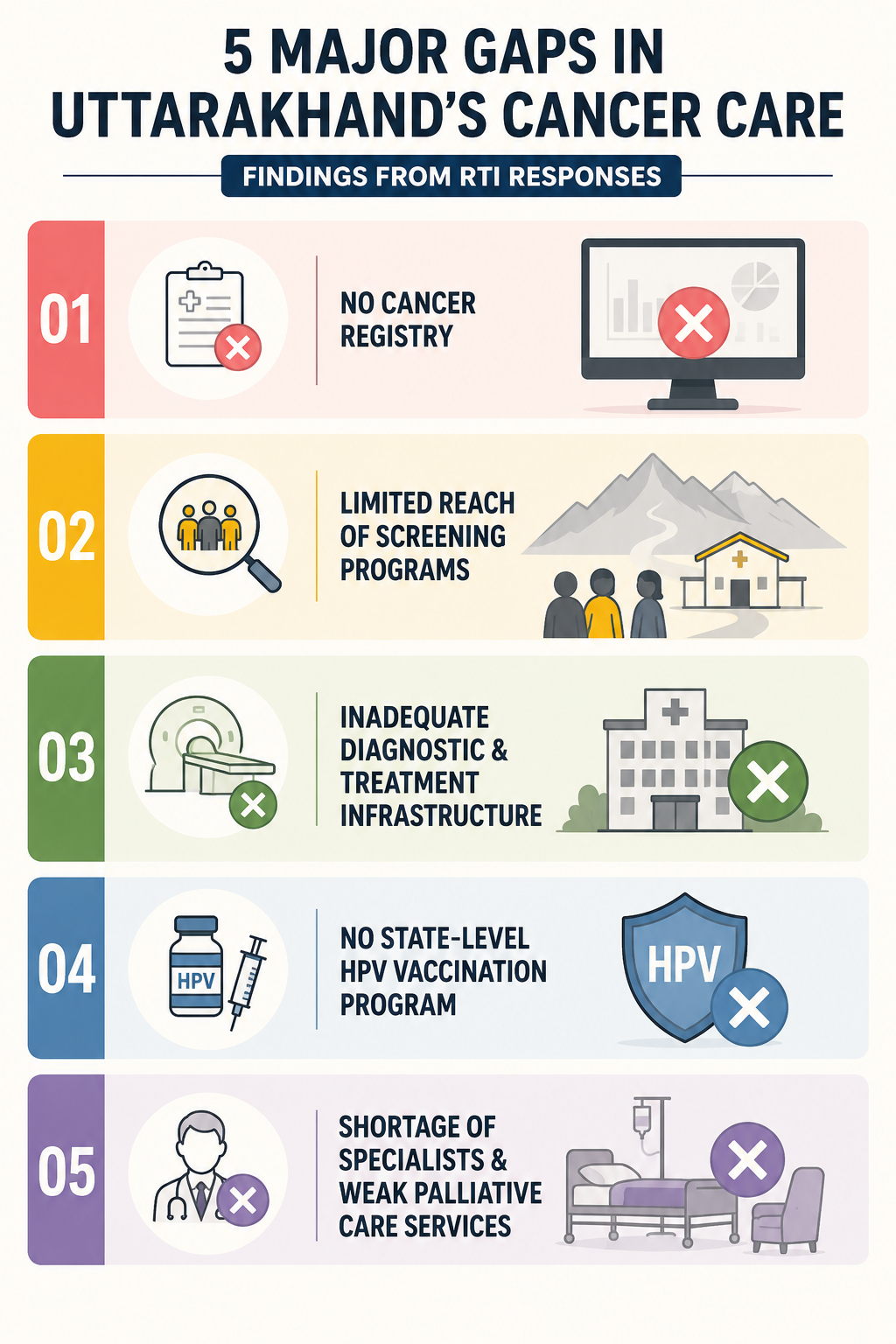
The RTI responses pointed to several serious gaps in Uttarakhand's cancer care ecosystem, raising concerns about the state's preparedness to deal with a growing burden of the disease.
Perhaps the most fundamental concern is the absence of a population-based cancer registry in Uttarakhand. Without reliable data on cancer incidence, mortality, and geographic distribution, policymakers are effectively operating in the dark.
One RTI response revealed that government hospitals in Nainital district recorded only a handful of cancer cases in 2024, while statewide screening camps detected just 13 cases during the same period. These figures appear inconsistent with the experiences of local communities, where cancer diagnoses have become increasingly common.
The lack of credible data raises a critical question: if the state does not know the true extent of the disease burden, how can it design evidence-based interventions to address it?
Although screening initiatives for breast, cervical, and oral cancers are being conducted, their reach appears limited. RTI responses indicate that only seven cases were detected through these screenings in 2024.
Rather than reflecting a low incidence of cancer, such figures may point to weaknesses in outreach, awareness, and access. Social stigma, limited awareness, logistical barriers, and the challenges of delivering healthcare in remote mountain regions continue to discourage participation, particularly among women.
The consequence is predictable: many cancers are detected only at advanced stages, when treatment becomes more difficult, expensive, and less effective.
Cancer diagnosis and treatment infrastructure remains concentrated in a few urban centres.
For example, according to RTI responses, Nainital district—an important referral hub for the entire Kumaon region—does not have a PET-CT scanner, a critical diagnostic tool used for cancer staging and treatment planning.
As a result, patients often travel hundreds of kilometres to cities such as Bareilly or Delhi for essential investigations, incurring significant financial and emotional costs. For many families, the burden of travel, accommodation, and repeated hospital visits becomes a major obstacle to continuing treatment.
Another important gap is the absence of a universal state-funded HPV vaccination programme.
The Human Papillomavirus (HPV) vaccine is widely recognised as one of the most effective tools for preventing cervical cancer, one of the leading causes of cancer-related deaths among women in India. Several states have already introduced free vaccination programmes for adolescent girls through public health systems.
Uttarakhand has yet to adopt a similar statewide strategy.
The state continues to face a chronic shortage of specialist doctors, particularly in its remote and hilly districts.
Recent RTI responses indicate that several specialist positions remain vacant, while many super-specialist posts—including oncologists and other experts needed to manage complex non-communicable diseases—have not been adequately created in accordance with healthcare norms.
This shortage reflects a long-standing failure in workforce planning and significantly limits access to specialised care.
The problem extends beyond treatment. Palliative care services, which play a crucial role in improving the quality of life of patients with advanced illnesses, remain poorly developed. RTI responses show that several districts lack dedicated cancer treatment facilities, while even existing palliative care units often struggle because of shortages of trained personnel.
Consequently, many patients and families are left to navigate some of the most physically, emotionally, and financially challenging periods of their lives with limited institutional support.
The challenges identified through RTI responses are not insurmountable. Across India, several states have adopted innovative approaches to cancer prevention, diagnosis, and treatment that Uttarakhand can learn from. Based on our findings, we submitted a representation to the Chief Minister, Health Minister, and senior officials in October 2025, highlighting the following priorities:
Uttarakhand should declare cancer a notified disease and establish a robust cancer registry system. Reliable data on incidence, mortality, and geographic distribution is essential for understanding the true scale of the problem and designing targeted interventions.
Without credible data, effective policymaking becomes difficult.
The state should implement a sustained, statewide cancer-screening programme, with particular emphasis on breast, cervical, and oral cancers.
Local NGOs, ASHA workers, self-help groups, and community institutions can play a critical role in raising awareness and encouraging participation. Experiences from states such as Kerala demonstrate that community-led approaches can significantly improve early detection.
Earlier diagnosis not only improves survival rates but also reduces treatment costs for families and the public health system.

Cervical cancer remains one of the leading causes of cancer-related deaths among Indian women.
In consultation with medical experts and public health specialists, Uttarakhand should evaluate the feasibility of introducing a free HPV vaccination programme for adolescent girls and other eligible age groups, similar to initiatives already adopted by several states.
One successful example is Australia, which is already on track to become the first country to eliminate cervical cancer, driven by a free school-based immunisation programme for students.
Preventive interventions of this nature have the potential to substantially reduce the future burden of cervical cancer.
Access to diagnostic and treatment facilities remains one of the largest barriers for cancer patients in Uttarakhand.
The state should invest in expanding PET-CT scanners, radiotherapy units, oncology services, and palliative care facilities across regions. Strengthening government medical colleges and major referral centres, particularly in Kumaon and Garhwal, would reduce the need for patients to travel long distances for essential care.
Health packages aimed at early cancer diagnosis, such as those implemented by the Tamil Nadu Government Multi Super Speciality Hospital (TNGMSSH), which have reduced the cost of cancer tumour marker tests to nearly one-tenth of that charged by private hospitals, could also improve access to early detection and timely treatment.
Infrastructure alone cannot improve outcomes without adequate human resources.
The state should create and fill specialist positions, including oncologists, onco-surgeons, gastroenterologists, and other critical specialists, particularly in underserved districts. At the same time, palliative care services must be expanded and adequately staffed.
Given that many patients currently travel outside the state for treatment, government support for travel, accommodation, and related expenses should also be strengthened. Such measures can reduce financial hardship and help ensure that patients continue treatment rather than abandoning it because of cost.
There are, however, some encouraging signs.
During an RTI appeal hearing in March 2026, senior health officials informed us that the Uttarakhand government had initiated the process of classifying cancer as a notifiable disease. In addition, the Governor of Uttarakhand launched the National HPV Vaccination Initiative for the prevention of cervical cancer in February 2026. These are important steps, and the Health Department, policymakers, healthcare professionals, and civil society groups advocating for better cancer care deserve recognition for pushing these issues onto the public agenda.
If implemented effectively, such measures could significantly improve cancer surveillance, prevention, and care delivery across the state.
At the same time, the broader healthcare challenges facing Uttarakhand cannot be ignored. While the state has made notable progress in areas such as maternal and child health, access to quality healthcare remains uneven, particularly in remote mountain regions where residents often travel long distances for basic and specialised medical services.
This reality was reflected in the recent healthcare movement in Chaukhutiya, Almora, where residents mobilised against the absence of essential medicines, diagnostic facilities, emergency care, and specialist doctors. What began as a local protest evolved into a larger public movement, culminating in a 300-kilometre march to Dehradun. The movement underscored a simple but powerful message: access to healthcare remains one of the most pressing development challenges in the state.
As Uttarakhand completes 25 years of statehood, this is not only a moment for celebration but also for reflection. Will the state continue to depend heavily on neighbouring regions for advanced medical care, or will it invest in building the institutional capacity needed to provide timely and quality treatment closer to home?
The answer matters because healthcare is not merely a welfare service; it is a foundation of human development. Without accessible and affordable healthcare, the promise of development remains incomplete.
Cancer may be the focus of this investigation, but the larger lesson extends beyond a single disease. Strengthening Uttarakhand's healthcare system will require greater public investment, long-term planning, and sustained political commitment. The costs of inaction are measured not only in statistics but in lives lost, families pushed into hardship, and patients forced to suffer in silence.
Zubair is a research scholar working on public health and equity issues and a resident of Nainital, Uttarakhand.
Liked this blog? We urge you to support our ongoing advocacy and research efforts by donating us online here:
